Take a Deep Breath: Understanding respiratory illnesses
Neil Trainis,
27 Feb 2025![]() 1 Min
1 Min
Neil Trainis,
27 Feb 2025![]() 1 Min
1 Min
Neil Trainis,
27 Feb 2025![]() 1 Min
1 Min

Respiratory illnesses, from the common cold to chronic diseases such as asthma and chronic obstructive pulmonary disease (COPD), are among the most common health issues. Steve Titmarsh explains…
Community pharmacists can play their part in educating people about these diseases and how to prevent them or minimise their impact on health.
The NHS Long Term Plan says respiratory disease affects one in five people in England and is the third biggest cause of death.1
🚩Key risk factors
According to the World Health Organization (WHO) common risk factors include:
**Asthma alone affects 5.4 million people in the UK.
The updated NICE guidelines3, published in November 2024, represent a collaboration between NICE, the British Thoracic Society (BTS) and the Scottish Intercollegiate Guidelines Network (SIGN). It highlights the importance of patient history in the diagnosis, partly as there is no accurate test yet for the disease.
Shift in diagnosis & treatment
Treatment
Monitoring is especially important and should be done at least once a year for people whose asthma is controlled, and more often if it is not. Seeing patients after an asthma attack is also key because attacks signal that treatment is not working.
NICE also recommends that inhaler technique should be checked at every opportunity – something pharmacists could do when dispensing inhalers.4
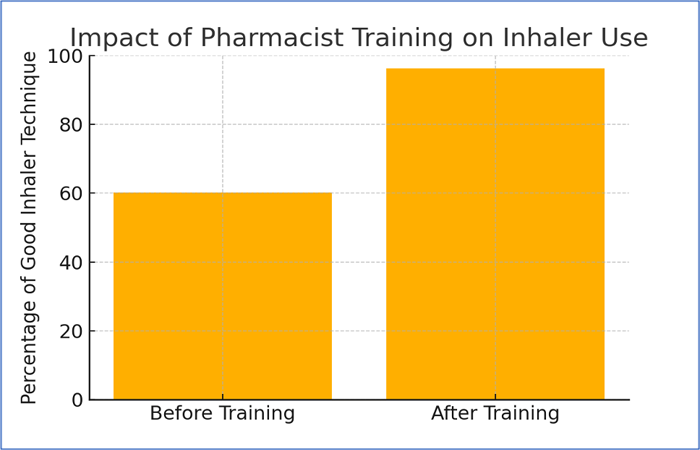
📊Study findings from Thorax:
A 2019 study of 380 patients with COPD or asthma recruited by 35 community pharmacies found:
➡️ Pharmacists play a key role in ensuring patients use inhalers correctly: Educating patients about their asthma and its treatment is important to equip them to deal with attacks and strategies to reduce the risk of attack by, for example, avoiding common triggers such as pollution.
In its submission to the government on healthcare workforce pressures, the British Thoracic Society (BTS) emphasised:
In its report A respiratory workforce for the future, the British Thoracic Society says:
“Exacerbations and frequent admissions to hospital are common to many respiratory diseases, for example COPD and asthma. Shifting the focus from reactive to proactive care has enormous benefit to patients and the healthcare system.”
“Supported self-management is a key part of the NHS Long Term Plan’s commitment to make personalised care the norm for patients. The narrative needs to change from admission avoidance to admission prevention.”
"To help deliver that part of the plan we will need to support community pharmacists in building confidence in advising patients with respiratory symptoms."
Darush Attar-Zadeh, a community pharmacist and Executive Committee member of the Primary Care Respiratory Society, wrote in 2019 a blog endorsing the role his colleagues can play in helping people with asthma. This included:
✅ Promoting good inhaler techniques
✅ Educating patients about medicines and what to expect from them
✅ Community pharmacists’ knowledge and skills can complement those of GPs managing people with respiratory diseases’, he said.7
In its handbook on chronic respiratory disease for pharmacists the International Pharmaceutical Federation (FIP) notes: as healthcare delivery undergoes a paradigm shift towards a people-centred care approach to optimising therapy and health outcomes, pharmacists are well positioned to play a unique and complementary role in an interprofessional collaborative care model to manage chronic respiratory diseases.8
Prevention
Community pharmacists can play a key role in helping to reduce the spread of respiratory infections by:
📊 Impact of the COVID-19 pandemic: In 2020, there was a 36% reduction in emergency asthma admissions. This was partly due to hygiene measures adopted during the peak of the pandemic, including encouraging people to stay home if they have a cold or the flu, and wearing a mask if they are with others.
Described by some as the first breakthrough in 50 years for treating asthma and COPD, a monoclonal antibody –benralizumab – made headlines in November 2024 following the results of a trial in people with severe asthma or COPD.10
What is benralizumab?
A trial published in November 2024 in The Lancet involved 158 patients who were randomly assigned to receive an injection of benralizumab or a five-day course of prednisolone or a combination of both. 90 days later:
🌟Benralizumab may offer a more effective alternative to steroids for managing eosinophilic asthma attacks
References